


To the Editor:
Q fever is considered a new and emerging zoonosis in The Netherlands since the first reported outbreak in late spring 2007 [Reference Karagiannis1]. In support of this hypothesis, Schimmer et al. [Reference Schimmer2] recently reported a low seroprevalence of 2·4% in The Netherlands in the period leading up to the outbreak (February 2006–June 2007) by retrospectively testing sera available from randomly selected municipalities throughout the country from the Dutch National Immunization Programme. However, the highly epidemic municipalities of 2007–2010 were excluded from the study sample, leaving unanswered the question whether Coxiella burnetii emerged as a genuinely novel infectious agent in those areas in May 2007.
We present here data from a retrospective study performed in the geographical epicentre of the first Q fever outbreak. The aim of the study was to investigate the aetiology of clinically treated pneumonia cases in the period leading up to the first reported outbreak. The outbreak's epicentre was located in the rural village of Herpen, in the province of Noord-Brabant. Herpen lies within the catchment area (catchment population: ~190 000) of the nearby located community-based Bernhoven Hospital in Oss.
We determined the contribution of C. burnetii as a causative agent of pneumonia in patients admitted for pneumonia to Bernhoven Hospital in the period January–July 2007. Pneumonia cases were identified retrospectively by retrieving all entries for ‘pneumonia’ from the hospital's electronic diagnosis registration system. A pneumonia case was defined by the presence of one or more clinical compatible symptoms (fever, cough, dyspnoea, headache) and a (new) infiltrate or consolidation on chest imaging (chest X-ray or CT scan).
If no causative agent had already been identified using standard cultures and serology, available sera were tested retrospectively for C. burnetii, using both complement fixation test (CFT) and PCR.
Of the total of 95 clinical pneumonia cases identified, C. burnetii was the causative agent in 21 (22%) patients. These patients showed a fourfold increase in CFT in paired samples. One Q fever patient had a positive serum PCR with negative CFT at presentation, but seroconverted in the follow-up CFT sample taken 3 months later.
In seven (7%) cases a pathogen other than C. burnetii was found, and in 23 (24%) cases no cause was found after serological testing. In the remaining 44 (47%) cases sera could not be obtained (Fig. 1). The mean number of pneumonia cases was 13 per month (range 5–29). The number (n=13) of Q fever pneumonia cases in May was significantly higher than in any other month in the study period (range 0–5) (P<0·05). For all other groups (other pathogen, unknown aetiology, no serology available), the number of cases did not differ significantly between months in the study period (P>0·05 for all groups). The contribution of C. burnetii as a causative agent of clinically treated pneumonia sharply increased in May 2007 compared to January–April 2007. There was no evidence of underreporting of Q fever pneumonia in the period leading up to the outbreak.
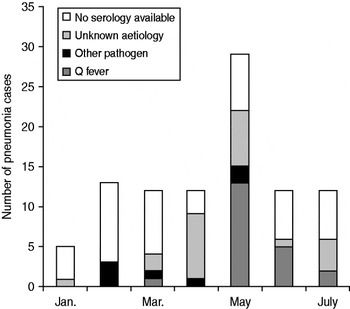
Fig. 1. Aetiology of pneumonia cases in Bernhoven Hospital in the period leading up to the first reported Dutch Q fever outbreak.
In order to examine these data further in a historical perspective, we retrieved data on number of pneumonia cases from the local diagnosis registration system from Bernhoven Hospital for 2005 and 2006. In the 2 years preceding the 2007 outbreak, the number of pneumonia cases was stable with expected seasonal variations in 2005 (206 cases) and 2006 (170 cases), but with no sudden sharp increase as was observed in 2007 (272 cases). This significant increase in number of pneumonia cases, especially in late spring and summer, further supports the notion of the introduction of C. burnetii as a new aetiological agent of pneumonia in this region.
A Q fever diagnosis can easily be overlooked as symptoms are non-specific and the clinical course is generally mild. In addition, sheer unfamiliarity with Coxiella burnetii as an infectious agent could have led to an underreporting of Q fever cases by attending physicians. Interestingly in this regard, Van den Wijngaard et al. [Reference Van den Wijngaard3] found retrospective statistical evidence of clustering of hospitalizations of possible and plausible Q fever pneumonia cases starting as early as 2005. However, lack of serological testing precluded definite confirmation of these outbreak clusters as being caused by Q fever.
Our data support the hypothesis that C. burnetii emerged as a novel aetiological agent of pneumonia in the epidemic area in The Netherlands in May 2007.
Declaration of Interest
None.

