


1 Introduction
Over the past few decades, China’s health care system has found itself to be increasingly subjected to negative comments. One persistent set of criticism argues that system-wide incentives, especially the under-subsidised health providers overly relying on provision of medical care and drug sales to survive, are identified as one fundamental cause for rapidly rising health care costs, medical impoverishment and unaffordable access (Yip and Hsiao, Reference Yip, Hsiao, Chen, Hu, Ma and Maynard2009: 613–619; Ramesh et al., Reference Ramesh, Wu and He2014).
Defined as the practice of over prescribing medicines, prescribing unnecessary and costly medicines, medical instruments and diagnostic procedures, ‘over-prescription’ is believed to lead inefficiency and poor quality in health care provision in China, and became a serious problem for the poor and the uninsured (Yang, Reference Yang2014; Yang and Wu, Reference Yang and Wu2014). A number of quantitative studies explored the causal relationship between provider incentives and over-prescribing practice; however, due to the nature of quantitative research, these studies were not able to provide an in-depth analyses of the issue of over-prescription or to enunciate the root causes of it (Yip and Eggleston, Reference Yip and Eggleston2004: 267–277; Wagstaff et al. Reference Wagstaff, Yip, Lindelow and Hsiao2005; Wagstaff and Lindelow, Reference Wagstaff and Lindelow2008: 990–1005; Yip and Hsiao, Reference Yip, Hsiao, Chen, Hu, Ma and Maynard2009: 613–619; Wagstaff et al., Reference Wagstaff and Yu2009: S7-S23; Babiarz et al., Reference Babiarz, Miller, Yi, Zhang and Rozelle2010; Babiarz et al., Reference Babiarz, Miller, Yi, Zhang and Rozelle2012: 1065–1074; Yang and Wu, Reference Yang and Wu2014). Several qualitative studies discussed the relationship between payment incentives and provider behaviours, but results by far are still anecdotal (Yip and Hsiao, Reference Yip and Hsiao2008: 460–468; Blomqvist and Qian, Reference Blomqvist and Qian2008: 5–26; Yip and Hsiao, Reference Yip, Hsiao, Chen, Hu, Ma and Maynard2009: 613–619).
A series of policy initiatives aiming at preventing over-prescription and correcting provider payment incentives were enacted in the 2000s, e.g. establishing drug purchasing mechanism, decoupling policy, zero mark-up policies (The State Council of P.R. China, 2015a, 2015b; Yi et al., Reference Yi, Miller, Zhang, Li and Rozelle2015: 1391–1398). Evidence on the effectiveness of these policy initiatives is largely mixed. In order to facilitate the discussion on developing effective and feasible policy initiatives to overcome the issue of over-prescription, it is important to understand the process of over-prescription, strategies that pharmaceutical companies employ to motivate health providers, and how this links to medical departments as well as medical doctors.
This paper seeks to provide an empirical investigation on the issue of over-prescription at four levels: hospital, medical department, doctors and pharmaceutical companies. It first examines various funding pressures hospital faces and how hospital transfers these pressures to medical department. It then looks at strategies developed by the medical department to cope with hospital level funding pressure, as well as how over-prescription is motivated and carried out in clinical settings. This paper also explores the growing interactions with hospital and pharmaceutical industry. This paper incorporates fieldwork data from the city of Shanghai, where 13 semi-structured face-to-face key informant interviews were conducted from 2008 to 2009.
This paper proceeds as follows. The first section describes data collection and methods. The second section described empirical results concerning over-prescription and how over-prescription was carried out at different levels, followed by a final section of conclusion and policy implications.
2 Methods
2.1. Data collection
Thirteen informants were interviewed over the period of 2008–2009. This study used the snowballing sampling technique to select informants. Eligible informants groups were medical doctors, pharmaceutical sales persons and hospital directors or department managers in hospitals. A main reason for focusing on these groups was to ensure that the issue of ‘over-prescription’ can be approached from a number of different perspectives to provide a balanced and holistic account. Medical doctors were interviewed in order to provide information on the economic pressures they face, the policy environment in which they operate and their understanding of what constitutes ‘good practice’ as far as prescriptions are concerned. Pharmaceutical sales persons employed in either international or domestic pharmaceutical companies were also interviewed. They were asked about the nature of their interaction and on-going relationship with medical doctors, the incentive system for employees in their firms and the techniques they employed to boost drug sales. Hospital directors or department managers interviewed included those involved in making and enforcing policies related to hospitals administration and, in particular, prescription drug dispensation. They were asked about questions related to prescription and hospital revenues, the interaction between hospitals and pharmaceutical companies, and their perceptions of the strengths and weakness of various health policies relating to hospital findings. Table 1 includes a profile of the informants.
Table 1 Key informants profile

The informant was asked for verbal consent about being a participant upon the start and the end of every interview. The process was supplemented by a Participant Information Sheet which included aims of the research and other details of rights of informants, such as confidentiality and freedom to terminate the participation at any point of time. Consent was obtained only after the informant fully understands the Participant Information Sheet. Participation is anonymous and confidential.
2.2. Analysis
Notes were taken during the interviews. Interviews were then transcribed. The transcribed data were coded thematically and analysed to discover emergent patterns and themes related to over-prescription. Specifically, interview data were grouped into four levels (e.g. hospital, medical department, doctors and pharmaceutical companies) as discussed in the introduction section. Data were then coded to identify themes and key findings for each level. Themes from each level were then used for generating an overall picture of the process of over-prescription. The themes were further elucidated by focussing on the process and root causes of over-prescription and its implications at different levels of stakeholders.
3 Empirical results
Thirteen in-depth interviews were conducted. The participants’ quotes are presented in italics. Considerable consistency between most interviewees’ accounts, including hospital directors, medical doctors and pharmaceutical sales representatives, was found. This section draws out the most important, commonly agreed themes across the different groups interviewed.
The process of over-prescription and over-use of health services can be understood from four interrelated level, i.e. hospital level, medical department level, doctor level and pharmaceutical company level. As illustrated in Figure 1, due to the insufficient funding from the government and rising operational costs, hospitals have to rely on the sales of drugs and provision of medical services to survive. This funding pressure then transferred to specific revenue targets for medical departments. A combination of incentives, including drug remunerations, bonus system, low pay and high workloads motivate over-prescription at doctor level. It is worth noticing that at pharmaceutical company level, high profits of pharmaceuticals products as well as lack of emphasis on efficacy of drugs leads to under-table payments and illicit drug remunerations. The following section provides detailed evidence of the process.
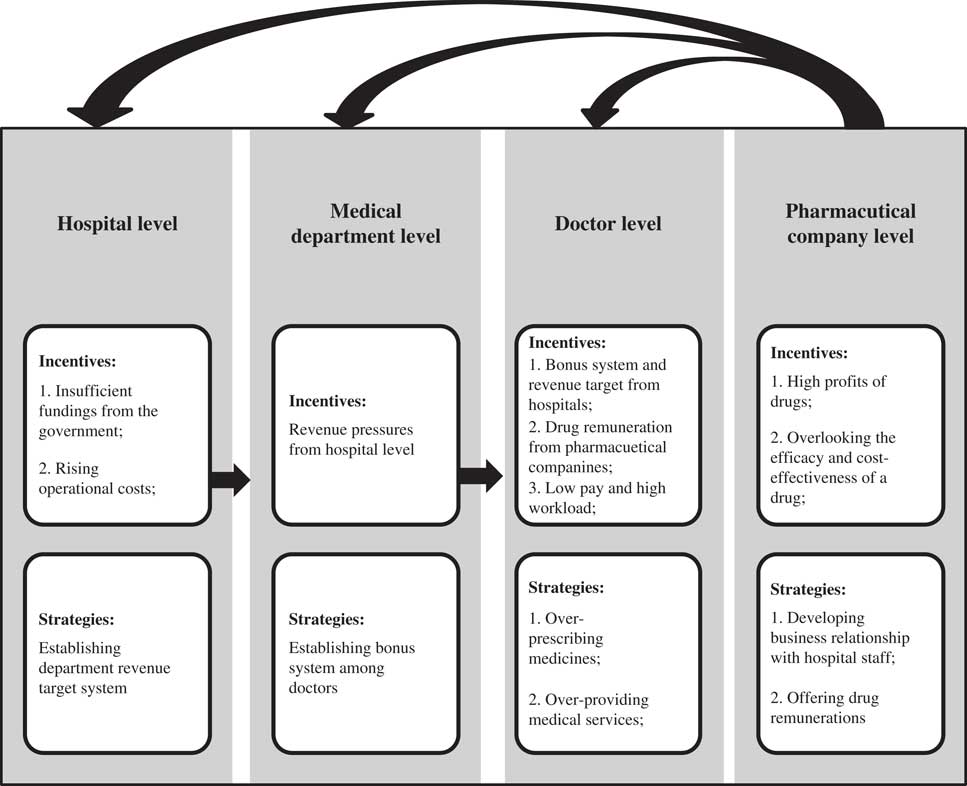
Figure 1 Incentives and strategies of different stakeholders
3.1. Funding pressures for hospitals
3.1.1. Insufficient funding from central and local governments
The first layer of incentives of over-prescription came from funding pressures that hospitals face. As suggested by the informants, hospitals revenues were mainly from two sources: government subsidies and user fees. The former partially covered capital, labour, and intermediate costs, and were subsidised by “central government, city government, and district government” (Hospital director). However, only a small fraction of total revenues were from by the government, as noted by a hospital director: “In my hospitals, only 20% of the total revenues are from the government; (revenues from) pharmaceuticals and medical service accounts for 50% and more…”
Funding pressure was suggested as one major financial difficulty faced by the hospital. One common problem raised by hospital directors was that the local government lack incentives to invest in health care sector because “health care is of low priority in local government’s funding agenda”. As noted by an informant:
I think the biggest problem is that there is not enough money for healthcare sector. It is also related to whether health care is a policy focus of the local government. I remember that in the past the government would allocate certain percentages (of their budget) to subsidise healthcare sector, but now it seems there is no such policy… At least in my district, hospitals are almost financially independent (Hospital director).
It was not uncommon to see that public hospitals faced financial difficulty. One informant revealed a story that a township health centre was “in great debt and was almost closed”. As he added: “Pharmaceutical companies refused to supply drugs. The government had to help the hospital to pay for the money they owed”. He also emphasised that “this is not a special case, and another hospital had similar problem in surviving” (Hospital director).
The accounts from the informants illustrated that funding issues were commonly faced by health facilities. Government subsidies were far from enough to support hospitals, and hospitals had to rely on other means to generate revenues.
3.1.2. Rising recurrent costs for hospitals
Apart from insufficient government subsidies, hospitals also encountered problems in coping with growing costs. Capital costs, which normally include building new wards, purchasing medical equipment and other related costs, constituted a significant proportion of the overall cost increase. As pointed out by an informant:
Related expenses are increasing… The profit (earned by the hospitals) actually dropped a lot…The space for hospital development is limited by not having enough money. As we all know, in order to expand, hospitals have plans for expanding the existing facilities and purchasing more medical equipment, but now hospitals have to pay for these themselves…We need to add depreciation costs for our equipment and other expenses…This was very difficult for most of district and township hospitals (Hospital director).
Informants also mentioned that labour costs were becoming increasingly expensive. A hospital director, noted: “According to the government’s policy, staff’s salary must increase every year. It has been really difficult for us. A lot of district hospitals are losing profits. Although the government subsidises us, it is not enough” (Hospital director).
Because of insufficient funding and growing running costs, many hospitals faced the problem of the shrink of the net profits, which led to the dreadful situation of under-funding. According to the informant:
Hospital revenue was 4-5 million RMB a few years ago. Now it is 8.5 million RMB. It seems that the revenues are increasing, but actually it is not true. The net profit is decreasing, because other related expenses are simply too expensive (Hospital director).
3.2. Setting sales target for individual medical departments
The responses from hospital directors suggested that the funding issue was a major problem for hospitals. Unsurprisingly, in order to compensate for the loss of health care subsidies and to secure enough funds for expansion and development, hospitals were encouraged to generate revenues from drug sales and provision of services. As indicated by a number of informants, the actual practice of making profits from pharmaceutical sales and care provision was through mechanisms of assigning revenue targets for medical departments, and linking doctors’ salary with bonus.
Generating sales revenues from pharmaceuticals and medical services was commonly referred as “using pharmaceuticals to feed hospitals” – a practice which all medical staff were aware of and made to follow. This is mainly because that costs for basic health services were set low, hospitals tend to over-prescribe or overuse diagnostic procedures to cross-subsidize the basic medical treatment. As suggested by a medical doctor:
We, healthcare practitioners all know ‘pharmaceuticals feed hospitals’. Most of the profits in hospitals are from the sales of pharmaceuticals and the provision of medical services. How much bonus we receive depends on how much pharmaceutical sales and medical services revenue we generate… Mostly it is the pharmaceuticals (that accounts for a large portion of the hospitals) (Medical doctor).
One noticeable strategy employed by most hospitals in Shanghai was to set up revenue targets for individual medical departments. As suggested by a number of informants, the revenue provided by each individual medical department’s were reviewed quarterly, which gave pressure for the manager as well as doctors in that department. One informant stated:
We have targets for each quarter, and we have to fulfil it to generate enough profits. There are regular meetings in the hospital. We discuss which medical department is not doing well in terms of meeting targets. We, doctors, all want to generate profits, and the hospital wants to generate more profits as well (Department manager).
Since each individual department had its own revenue target, doctors were encouraged to prescribe more drugs or to encourage the patients to undergo thorough physical examines in order to fulfil the hospital targets. Another informant also provided similar account: “The income of the department is from drug prescription and the provision of medical services. In order to fulfil the department target, we will encourage most patients to undergo thorough physical examinations before any diagnoses are made. This is required by the department’” (Medical doctor).
3.3. Incentives for over-prescription for medical doctors
3.3.1. Hospital bonus system
At the doctor’s level, vigorous mechanisms were established in conformity with the funding issues. Apart from the salaries, doctors received bonus, which was linked to the amount of drugs they prescribed and revenues generated by the medical department. As noted by a doctor:
My bonus is associated with the performance of the department…My bonus was paid quarterly. This quarter is around 2500RMB; sometimes I receive more if the department target is met… (Medical doctor).
Similar account was provided by a surgeon. The average bonus for his department was “higher compared with other department” because they usually “had more patients than others”. He also mentioned that doctors in some departments, e.g., Orthopaedics, may “receive even higher bonus because they have more patients”. The amount of bonus a doctor earns can be up to “twice as much as the basic salaries” (Medical doctor).
The responses from the doctors demonstrated how a mechanism had been set up to motivate prescription. Hospitals can barely maintain or develop itself if it did not provide care for profits. Sales of pharmaceutical products and provision of services became hospitals’ strategies to generate profits and to guarantee patient flow, which was based on the profit-seeking principle rather than on fulfilling its social functions.
3.3.2. Use bonus and drug remunerations to compensate low pay
One important reason for the bonus system to work was because that bonus constituted a significant proportion of doctor’s income. A number of medical doctors expressed their discontent towards their salaries. Most of them agreed that their salary level cannot reflect their knowledge and skills. Their salaries were “low” compared with people who “worked for private companies”. Some of them also think that their work was “labour-intensive” given the fact that “it was common to do night shifts”. As suggested by a surgeon:
I am always very busy at work. I have so many patients to attend to. It is common for me to do a 5-6 hours operation. The hospital always calls me for emergency situations because they cannot find any senior people (Medical doctor).
When being asked about the salaries, the informant expressed discontent:
My basic salary is around 4600RMB per month. I know this basic salary is the same for all doctors in Shanghai hospitals at my level and working experience. Given the high living costs in Shanghai… the basic salary is not enough to pay for a decent life
Similar account was provided by a medical doctor:
(Medical doctors) is a job that requires years of training and deals with lots of risks. But their salaries, compared with their foreign counterparts are quite low… People laughed at them and said, ‘scalpels do not even value as much as a barber’s scissors’. Do you think this is fair?
The narratives provided by the informants suggested that there was a general discontent among the doctors towards their basic salaries and high workloads. Most of the informants agreed that their basic salaries should increase to match with the training they had and the workload of their jobs.
3.4. Incentives from pharmaceutical companies
3.4.1. High profits of pharmaceutical products
As commonly noted by the medical doctors and pharmaceutical companies, drugs were still priced high in terms of the actual costs. Pharmacies owned and run by hospitals were allowed to sell drugs at a mark-up of 15% and these profits were non-taxable. As noted by another informant:
Hospitals receive most of the profit (from drug sales). For example, the cost for producing a bottle of N (a name of a western medicine) is about 4RMB, we sell it to our distributors at a price of 28.77RMB. The hospital sells it at 40RMB (Pharmaceutical sales representative).
Similar accounts were provided by another informant:
Generally, the profit of a drug could be divided into three parts. The profit for the pharmaceutical company is around 5-15% of the wholesale price, and 10-30% for the hospital (Pharmaceutical sales representative).
It is also noted that because of the high profit margin of drugs, most pharmaceutical sales representatives have a budget known as “promotion budget” or “clinical budget”, which can be used for “developing business relationship with hospital staff”, “paying drug remunerations”, and other drug promotion methods (Pharmaceutical sales representative).
3.4.2. Developing business relationship with hospital staff
In order to market their drugs, pharmaceutical sales representatives approach doctors by using their personal connections. Common strategies as mentioned by the informants included “ask friends, relatives, colleagues and classmates to introduce them to doctors, and it was often very difficult to for the doctor to refuse to see them” (Hospital director).
Informants from pharmaceutical sectors suggested that maintaining a personal relationship with medical staff was the key to promote the sales of their products. Sales persons often treated doctors as close friends, and socialised them after work. They knew their families and helped to manage matters even these are unrelated to their work. As learned from a pharmaceutical sales representative:
Most of the time, my job is to deal with medical doctors. I approach them, introduce the drugs to them. I need to know their needs, their family, even their personal likings. I give them presents, money or other things that will please them, hoping that they will prescribe more medicines from my company not others (Pharmaceutical sales representative).
Another pharmaceutical sales representative stated:
As for me, I gave doctors cash, sometimes other gifts. It depends on the doctors; I heard my colleague even bought branded skin care products for female doctors (Pharmaceutical sales representative).
Strategies used by pharmaceutical companies to maintain business relationship with doctors included “playing pokers with them” and “picking up their kids from school” (Pharmaceutical sales representatives).
The responses from the informants showed that pharmaceutical sales persons were persistent in approaching medical doctors and promoting their products. Interestingly, none of these informants mentioned about the efficacy of their medicines. The nature of their work was to maintain a good relationship with doctors and to sell drugs rather than promoting the drugs for their efficacy.
3.4.3. Offering drug remunerations
The most widely adopted strategy by pharmaceutical companies to motivate prescription was to offer direct drug commissions on each prescription. However, in order to sell drugs in a hospital, the approval of the Hospital Pharmaceutical Committee (yao shi wei yuan hui) was required. The committee is usually “comprised of the director of the pharmacy department, the vice hospital president, directors from various medical departments, and some other specialists” (Pharmaceutical sales representative). Decisions made by these individuals were crucial in determining whether the drug can be sold in the hospital. Pharmaceutical sales persons offered members of the pharmaceutical committee money or gifts to establish a good personal relationship. As noted by a pharmaceutical sales representative:
The most important thing is to know who are the key persons in the committee (Hospital Pharmaceutical Committee)… Targeting the right persons is the key. The second step is to persuade the persons to speak for you at the meeting. We offer money… It is possible that the first time they will reject you… in the end, they will accept your money (Pharmaceutical sales representative).
Approaching key figures from the hospital pharmaceutical committee and persuading them to use the drugs in their hospitals was important, and a common strategy is to offer them economic incentives. A pharmaceutical sales representative provided a similar account:
We need to make sure that my company is maintaining a good relationship with these people (members from Pharmaceutical Committee), and offering money to them…. Some medicines need a lot of money to get listed in a hospital, especially for Chinese medicines (Pharmaceutical sales representative).
After a drug was listed in a hospital, the next step was to convince doctors to prescribe it. The most widely adopted strategy by pharmaceutical companies was to offer medical doctors drug commissions on each prescription. As noted by a pharmaceutical sales representative, a large proportion of doctor’s income could come from drug remunerations,
In Shanghai, a doctor work in outpatient clinics in a Class III hospital Footnote 1 can earn up to 50,000RMB a month from pharmaceutical companies. Drug remunerations are paid monthly based on how much the doctor prescribes (Pharmaceutical sales representative).
Aside from drugs, remunerations from medical device are also lucrative. A pharmaceutical sales representative gave a vivid example of how remuneration is paid:
Commissions for imported intravascular stents are around 2000RMB per unit… Some patients need more than one intravascular stents, maybe four or five stents…Usually commissions are around 20% of the listed price. We give the commissions to the whole surgery team, and let them split the money themselves…Commissions for domestic intravascular stents can be up to 40% of the listed price….
Other ways of offering drug remunerations included “fees for inviting doctors to give lectures” (Pharmaceutical sales representative). As suggested by pharmaceutical sales representatives, drugs remunerations can also be paid through other means. For instance, instead of offering direct cash payment, drugs remunerations were often paid in the form of fees for academic lecture:
Sometimes, a doctor does not need to give a lecture. We issue a receipt under a title of ‘fees for academic lectures’. We will transfer the money to the doctor as a way to pay for drug remunerations. This way, everything is legal (Pharmaceutical sales representative).
Doctors were also asked whether they knew or even accepted any drug remunerations. Some of them said that they never accepted drug remunerations. Some of them insisted that the prescription was based on the efficacy of the drug rather than remuneration, and drug remunerations did not influence prescription decisions. Others pointed out that some doctors may prescribe for remunerations:
The point is the profit is just there. Even doctors do not take it; the money will go into the sales’ pocket. However, there are some medical doctors who are deeply corrupted. For some personal profit, they will harm the patients…Doctors may choose to use the most expensive medical products and imported medicines just for drug remunerations. But not all of us will do it (Department manager).
These responses suggested that accepting drug remunerations was a common practice in Chinese hospitals, and drug remunerations can take various forms. Even though accepting any form of drug commission may be illicit, it was widely adopted.
3.4.4. Overlooking the efficacy and cost-effectiveness of pharmaceutical products
The prescription of drug should depend on the efficacy of the product, but responses from pharmaceutical sales representatives seldom mentioned about the efficacy of their products. For instance, branded drugs were usually much more expensive than the generics after the patent expires. As noted by a pharmaceutical sales representative, the most common strategy is to “offer doctor remunerations” to encourage the prescription branded drugs, even though “the efficacy of the drugs are same” (Pharmaceutical sales representative).
One commonly noted theme is that not all drugs were prescribed at a cost-effective manner. Pharmaceutical products with mild medical clinical effects, such as “vitamins”, “amino acid”, and some “Chinese herb medicines” were often recommended by the doctors. A pharmaceutical sales representative gave an example for the prescribing traditional Chinese medicines and medicines for recovery.
The most widely used medicine in my company is X. It could be used on a lot of diseases, for recovery. Drug remuneration is around 20% of the retail price… You may not need it, but anyway, it will not kill you (so doctors will prescribe it)… (Pharmaceutical sales representative).
Interestingly, most pharmaceutical companies did not see their marketing strategies as inappropriate or illicit. A pharmaceutical sales representative noted:
I do not think drug remuneration practice is wrong. Look at these products listed in supermarkets. A good merchandising also needs merchandising fees to put their products in the best place on shelf. It is the same with drug sales. The major difference between drug sales and products in a supermarket is that the decision of what drug to prescribe is made by the doctor. Because of this, pharmaceutical salesman needs to do whatever he can to persuade the doctors to sell the drug (Pharmaceutical sales representative).
The arguments made by these pharmaceutical sales representatives rested largely on the point that selling drugs was a business similar to selling products in a supermarket. Efficacy of the drug was largely overlooked, and most of the marketing strategies were based on the economic incentives of drug prescription.
3.5. Policies aiming at regulating drug remunerations
It would be unfair to say that the government has no intention to regulate the troubled pharmaceutical market. As health care costs increase dramatically, the Chinese government is determined to cut health care costs by focusing on over-priced drugs. The drug policy reform aimed at controlling health care cost emerged as a significant force shaping China’s pharmaceutical industry and ways of drug marketing. A set of complex and comprehensive policies towards pharmaceutical products and pharmaceutical industries were established.
The launch of the ‘Drug Purchasing Mechanism’ was a good example. Drugs with the same chemical formula needed to go through a ‘Purchasing Mechanism’, and those had the lowest prices can be listed in hospital. The purchasing mechanism was designed to reduce hospital administrators’ backdoor dealings when purchasing from drug companies. Besides, it was believed that doctors would have less commercial incentive to over-prescribe or to choose costly medicines over affordable ones when having fewer options of pharmaceutical products listed in hospitals.
Unsurprisingly, the implementation of the policy was also sluggish and difficult, because “the reduction of retail prices harmed the interest of the hospitals and the pharmaceutical companies” (Hospital director). In response to the purchasing mechanism, pharmaceutical companies developed strategies to response to the price control, such as “changing the regular product package”, “Reducing the doses of the tablets in order to make the prices look smaller”, which make the prices very difficult to compare (Pharmaceutical sales representative).
Another policy initiative was to require hospitals to decouple drug sales from hospital revenue, and to distinguish between drug revenue and profit earned through medical services. The intention of the policy was to channel resources away from pharmaceutical sales, especially costly imported pharmaceuticals, into medical services in order to improve the quality of health care and prevent corruption in hospitals. Ironically, health care costs, especially pharmaceutical costs, continued to climb although the share of pharmaceutical revenue appeared to shrink. As noted by the informants, instead of prescribing fewer drugs, most hospitals increased the use of medical services and high-tech diagnostic tests to balance the share between the pharmaceutical sales and medical services. As one informant noted:
Pharmaceutical revenue is the major source for the hospitals income…hospital revenue includes pharmaceutical income, diagnostic procedures fee, and basic fees… If pharmaceutical revenues are cut down, then we have to increase other fees or increase the use of other services, such as the use of various diagnostic procedures. This is what is happening now, and the healthcare costs will continue increase and remain high (Medical doctor).
Similar accounts were provided by a government official:
Who dares to say it is a wrong policy (decoupling policies)? In order to follow the policy and to keep the profit of the hospital, hospitals may promote use of high-tech diagnostic procedures, special wards and other methods to increase non-pharmaceutical expense…but this does not really mean the total cost of health care is decreasing (Medical doctor).
When asked whether such illicit practice can be regulated, an informant noted:
How to prevent the drug commissions? We have tried all what we can. You know, what drug doctor prescribe sometimes have some influence on hospital’s interest. If he prescribes more imported drugs, hospitals receive more profits. In this sense, hospitals do not have such motivation to regulate drug prescription (Hospital director).
This response showed that since drug sales are important to the hospital, hospitals have less incentive to regulate the inappropriate prescription. Hospitals can barely maintain or develop itself if it did not provide care for profits.
4 Discussion and conclusion
This paper provided an empirical investigation of the issue of over-prescription based on interview data from hospitals in Shanghai. Funding pressures translated into hospitals revenue regardless of efficacy or efficiency of prescription. Hospitals set revenue target for individual medical department and bonus schemes for doctors. Moreover, the business ties between the pharmaceutical companies and hospitals were even closer than before; the two interacted in a reciprocal manner to motivate drug prescription among patients to mutually benefit both parties. This study argued that the way that the Chinese health care system operates was based on the profit-seeking principle because the system can barely maintain or develop itself if it did not provide care for profit.
Over-prescription and its link with provider payment incentives has been documented in a number of studies. A study of the use of medicines in Tuberculosis (TB) treatment reported that pressure from the doctors to generate revenue through selling medicines and services was one main reason that some TB patients fail to have access to treatment (Liu et al., Reference Liu, Thomson, Gong, Zhao, Squire, Tolhurst, Zhao, Yan and Tang2007: 1464–1471). Ng (Reference Ng2011: 428–439), using data in hospitals in Guangdong Provinces from 2004 to 2008, suggested that unnecessary care, over-prescription of drugs, and the adoption of high-tech treatments were common practice to drive revenues. Similarly, a study conducted in Beijing, Gansu, Shandong, and Henan showed that hospitals still regarded high-tech diagnostic services as profitable, and overuse of expensive treatment was still prevailing (Eggleston et al., Reference Eggleston, Ling, Meng, Lindelow and Wagstaff2008). Similar findings were also demonstrated by Reynolds and McKee (Reference Reynolds and McKee2009: 32–36), who found that the treatment of common colds using injected medications of no therapeutic relevance has been fostered by the profit-led financing mechanism of the Chinese hospitals. Liu et al. (Reference Liu, Gao and Rizzo2011: 28–41) suggested that about 30% to 40% of drug consumption were deemed as inappropriate and were prescribed in an attempt to generate revenue for the hospital. Yang and Wu (Reference Yang and Wu2014) also found that the availability of insurance increased per episode costs for outpatient care; this increase was more pronounced among village clinics and township health centres – the backbone of the health system for rural residents – than at county and municipal hospitals.
The problem of over-prescription and overly use of health services in hospitals deserve attention. It may seem appealing for the government to simply inject more funding to the health care sector. However, the danger is that provider behaviours that escalate costs may again necessitate further subsidies. Scholars suggested a few potential packages for correcting incentives of over-prescription, which include drug price control, strengthen provider-payment reforms, improving provider management, etc. (Yip and Hsiao, Reference Yip, Hsiao, Chen, Hu, Ma and Maynard2009: 613–619; Wagstaff et al., Reference Wagstaff and Yu2009: S7-S23; Ramesh et al., Reference Ramesh, Wu and He2014; Yip et al., Reference Yip and Hsiao2012: 833–842). Yet, in the case of China, even though the government is well aware of such problem and has launched several policy initiatives to control it, these initiatives have met with little success (Eggleston et al. 2008). For instance, a study assessing the ‘decoupling policy’ which aimed to decouple drug sales from hospital revenues showed that the reform was not successful. Drug costs increased rapidly soon after the reform, since hospitals were able to shift the drug costs to other costs that were not controlled. The study concluded that improvement of rational use of drugs and correcting the incentive structure for hospitals and medical doctors were important to contain costs (Meng et al., Reference Meng, Cheng, Silver, Sun, Rehnberg and Tomson2005: 185–196). Zero mark-up of drug profit was launched in a number of provinces to squeeze the excessive profits in drug sales. However, evidence showed that although reduction in drug revenues was observed during the study period, costs for other health services increased, this was mainly because health care providers found new, potentially inappropriate, forms of revenue—service provision—to compensate for the loss of drug profits (Xu, Reference Xu2010: 336; Zhang et al., Reference Zhang, Liu, Chu and Li2014: 6; Wang and Cai, Reference Wang and Cai2015: 56; Yi et al., Reference Yi, Miller, Zhang, Li and Rozelle2015: 1391–1398). Evidence on the effectiveness of Centralised Drug Purchasing Mechanism, which was introduced to promote competitions among pharmaceutical companies and control drug prices, were also mixed. Scholars argued that hospitals still wield great power in deciding what drug to be used in their pharmacies because not all drugs need to go through the purchasing process (Peiming et al., Reference Peiming, Lili and Shumei2010: 51; Wang et al., Reference Wang, Mao and Du2015: 21). Moreover, the pilot policy interventions of clinical pathway reform, which was introduced as an instrumental to increase efficiency in resource use and control costs, also appeared to be ineffective (He and Yang, Reference He and Yang2015: 394–411).
The Chinese government seems to be ambitious about reforming the current health care delivery system and to provide a more adequate health care system backed by more budgetary resources. However, for the various health care policies, campaigns, and mechanisms initiated in the past two decades aiming at overcoming provider payment incentives and containing drug costs, very few has been effective. The successful implementation of any effective policies is reliant on the government’s determination to correct the endogenous structural problem of the health care system, and initiate a thorough reform of provider payment incentives – the fundamental causes for the sluggish implementation of most health policies. The decreased reliance on government funding, decentralisation of health care services, increased autonomy of health providers, and lack of effective regulatory framework in the local government further complicate the scenario. How to motivate the local and regional bureaucrats to effectively implement the legal stipulations to regulate provider behaviours, and how to regulate the pharmaceutical industry, are core questions that remain unanswered.
The study results need to be interpreted in light with the limitations. The scope of the research is limited to interviews of health care stakeholders and their narrative accounts. Although the issue of over-prescription has been widely noted in the context of China’s health care system, the scope of the study is limited to Shanghai. Therefore, any generalisations of the study finds should be made with caution.


